
Page 19 - 2021 Summer Enrollment
P. 19
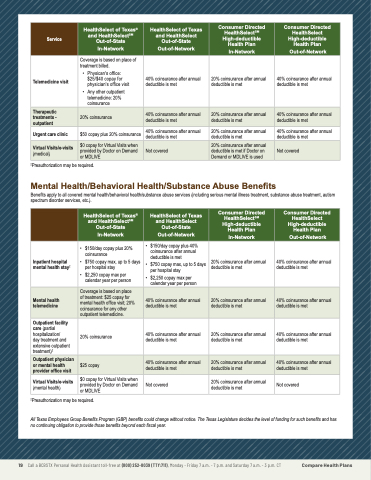
Service
HealthSelect of Texas® and HealthSelectSM Out-of-State
In-Network
HealthSelect of Texas and HealthSelect Out-of-State
Out-of-Network
Consumer Directed HealthSelectSM High-deductible Health Plan
In-Network
Consumer Directed HealthSelect High-deductible Health Plan
Out-of-Network
Telemedicine visit
Coverage is based on place of treatment billed.
• Physican's office: $25/$40 copay for physician's office visit
• Any other outpatient telemedicine: 20% coinsurance
40% coinsurance after annual deductible is met
20% coinsurance after annual deductible is met
40% coinsurance after annual deductible is met
Therapeutic treatments - outpatient
20% coinsurance
40% coinsurance after annual deductible is met
20% coinsurance after annual deductible is met
40% coinsurance after annual deductible is met
Urgent care clinic $50 copay plus 20% coinsurance 40% coinsurance after annual 20% coinsurance after annual 40% coinsurance after annual deductible is met deductible is met deductible is met
2Preauthorization may be required.
Mental Health/Behavioral Health/Substance Abuse Benefits
Benefits apply to all covered mental health/behavioral health/substance abuse services (including serious mental illness treatment, substance abuse treatment, autism spectrum disorder services, etc.).
Virtual Visits/e-visits
(medical)
$0 copay for Virtual Visits when provided by Doctor on Demand or MDLIVE
Not covered
20% coinsurance after annual deductible is met if Doctor on Demand or MDLIVE is used
Not covered
HealthSelect of Texas® and HealthSelectSM Out-of-State
In-Network
HealthSelect of Texas and HealthSelect Out-of-State
Out-of-Network
Consumer Directed HealthSelectSM High-deductible Health Plan
In-Network
Consumer Directed HealthSelect High-deductible Health Plan
Out-of-Network
Inpatient hospital mental health stay2
• $150/day copay plus 20% coinsurance
• $750 copay max, up to 5 days per hospital stay
• $2,250 copay max per calendar year per person
• $150/day copay plus 40% coinsurance after annual deductible is met
• $750 copay max, up to 5 days per hospital stay
• $2,250 copay max per calendar year per person
20% coinsurance after annual deductible is met
40% coinsurance after annual deductible is met
Mental health telemedicine
Coverage is based on place of treatment: $25 copay for mental health office visit; 20% coinsurance for any other outpatient telemedicine.
40% coinsurance after annual deductible is met
20% coinsurance after annual deductible is met
40% coinsurance after annual deductible is met
Outpatient facility care (partial hospitalization/
day treatment and extensive outpatient treatment)2
20% coinsurance
40% coinsurance after annual deductible is met
20% coinsurance after annual deductible is met
40% coinsurance after annual deductible is met
Outpatient physician or mental health provider office visit
$25 copay
40% coinsurance after annual deductible is met
20% coinsurance after annual deductible is met
40% coinsurance after annual deductible is met
Virtual Visits/e-visits $0 copay for Virtual Visits when 20% coinsurance after annual
(mental health) provided by Doctor on Demand Not covered deductible is met Not covered
or MDLIVE
2Preauthorization may be required.
All Texas Employees Group Benefits Program (GBP) benefits could change without notice. The Texas Legislature decides the level of funding for such benefits and has no continuing obligation to provide those benefits beyond each fiscal year.
19 Call a BCBSTX Personal Health Assistant toll-free at (800) 252-8039 (TTY:711), Monday - Friday 7 a.m. - 7 p.m. and Saturday 7 a.m. - 3 p.m. CT Compare Health Plans
