
Page 16 - 2020 Summer Enrollment
P. 16
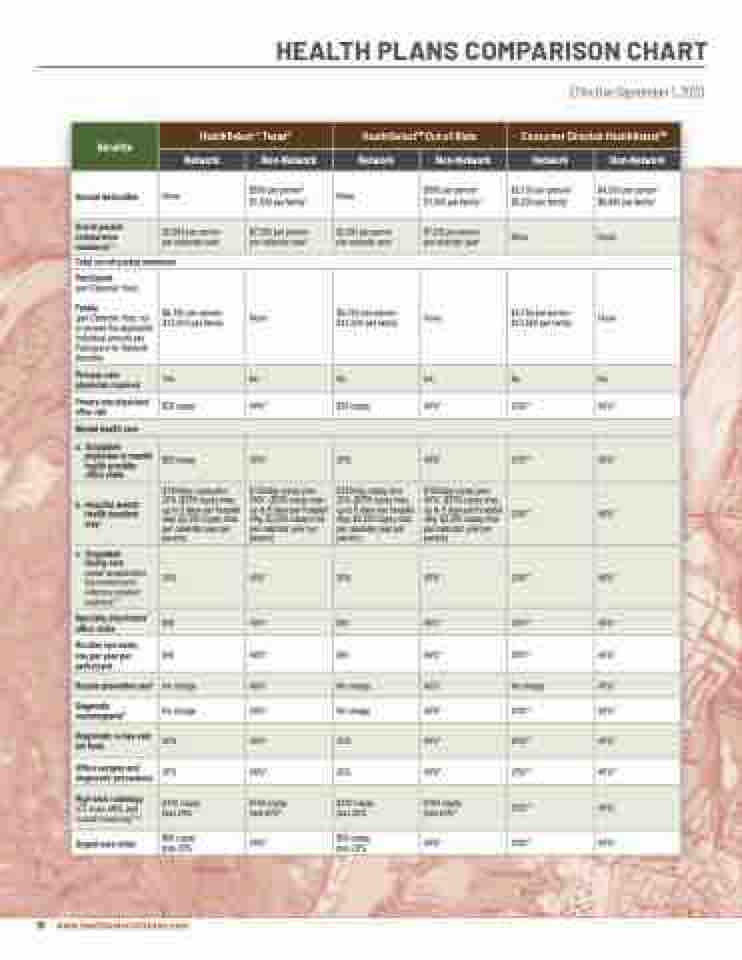
HEALTH PLANS COMPARISON CHART
Employee and Non-Medicare-Eligible Retiree
HEALTH PLANS COMPARISON CHART
Effective September 1, 2017
Effective September 1, 2020
Benefits
HealthSelectof Texas®
HealthSelectSM Out-of-State
Consumer Directed HealthSelectSM
Network
Non-Network
Network
Non-Network
Network
Non-Network
Annual deductible
None
$500 per person1 $1,500 per family1
None
$500 per person1 $1,500 per family1
$2,100 per person1 $4,200 per family1
$4,200 per person1 $8,400 per family1
Out-of-pocket coinsurance maximum2,3
$2,000 per person per calendar year1
$7,000 per person per calendar year1
$2,000 per person per calendar year1
$7,000 per person per calendar year1
None
None
Total out-of-pocket maximum
Participant
(per Calendar Year)
Family
(per Calendar Year, not to exceed the applicable Individual amount per Participant for Network Benefits)
$6,750 per person $13,500 per family
None
$6,750 per person $13,500 per family
None
$6,750 per person $13,500 per family
None
Primary care physician required
Yes
No
No
No
No
No
Primary care physicians’ office visit
$25 copay
40%*
$25 copay
40%*
20%**
40%*
Mental health care
a. Outpatient physician or mental health provider office visits
$25 copay
40%*
20%
40%*
20%**
40%*
b. Hospital mental health inpatient stay9
$150/day copay plus 20% ($750 copay max, up to 5 days per hospital stay. $2,250 copay max per calendar year per person)
$150/day copay plus 40%* ($750 copay max, up to 5 days per hospital stay. $2,250 copay max per calendar year per person)
$150/day copay plus 20% ($750 copay max, up to 5 days per hospital stay. $2,250 copay max per calendar year per person)
$150/day copay plus 40%* ($750 copay max, up to 5 days per hospital stay. $2,250 copay max per calendar year per person)
20%**
40%*
c. Outpatient
facility care
(partial hospitalization/ day treatment and extensive outpatient treatment)7,9
20%
40%*
20%
40%*
20%**
40%*
Specialty physicians’ office visits
$40
40%*
$40
40%*
20%**
40%*
Routine eye exam, one per year per participant
$40
40%*
$40
40%*
20%**
40%*
Routine preventive care#
No charge
40%*
No charge
40%*
No charge
40%*
Diagnostic mammograms#
No charge
40%*
No charge
40%*
20%**
40%*
Diagnostic x-rays and lab tests
20%
40%*
20%
40%*
20%**
40%*
Office surgery and diagnostic procedures
20%
40%*
$100 copay plus 40%*
20%
40%*
20%**
40%*
High-tech radiology
(CT scan, MRI, and nuclear medicine)7,8,9
$100 copay plus 20%
$100 copay plus 20%
$100 copay plus 40%*
20%**
40%*
Urgent care clinic
Chart_2017_Comparison
$50 copay plus 20%
40%*
$50 copay plus 20%
40%*
20%**
40%*
5/26/2017
16 www.healthselectoftexas.com
